
I’ve been working on a theory about how stigma causes violence.
 I started thinking about such a thing because, well, I’m a criminologist. My work involves people with mental illness (including bipolar disorder) who are involved in the criminal justice or legal systems, some who have been violent when they were unwell. Several of these stories have received special attention by the news media, usually with jaw-dropping headlines (e.g., Mentally Ill Man Murders Mother’s Mother).
I started thinking about such a thing because, well, I’m a criminologist. My work involves people with mental illness (including bipolar disorder) who are involved in the criminal justice or legal systems, some who have been violent when they were unwell. Several of these stories have received special attention by the news media, usually with jaw-dropping headlines (e.g., Mentally Ill Man Murders Mother’s Mother).
Of course, such incidents, including the news coverage, reflect badly on mental illness. They fuel the widespread belief that people with mental illness are ticking time bombs. It’s clear that violent acts committed by people with mental illness, regardless of how infrequently they occur, contribute to stigma. Dr. Torrey outlines this point in a provocative article called “Stigma and Violence: Isn’t it Time to start connecting the Dots1.”
As I was reading this article about how untreated mental illness and violence causes stigma, I was stunned by the solution offered up by the author. His method for reducing the stigma associated with mental illness was [insert dramatic pause] compulsory treatment. Really?!
I can see his point that reducing the incidence of violent acts committed by people with untreated mental illness might improve public attitudes and beliefs (aka social stigma). However, I’ve spoken to lots of people (i.e., hundreds) who have been involuntarily hospitalized, forcibly medicated, and had their freedoms restricted in the community2. For the most part, compulsory treatment has not enhanced the extent to which they feel included and valued by society (aka self-stigma).
For me, something isn’t quite right with the idea that compulsory mental health treatment reduces stigma. I have been trained to be highly suspicious of any simplistic formulations of complex social problems. So, I took out my notepad and started sketching what I know about the relationship between stigma and violence. Here’s what I came up with:
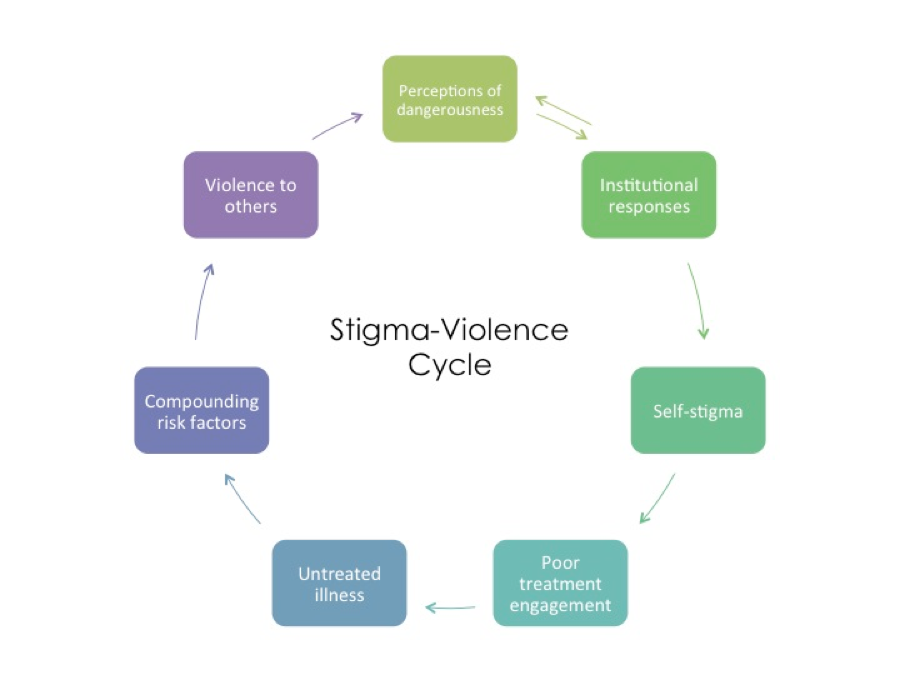
This theory offers a much different version of events, which I’ll briefly summarize. Starting at the top, public perceptions that dangerousness is a key characteristic of mental illness triggers the government to respond by creating laws (aka institutional response) that restrict the rights and freedoms of people with mental illness. These laws enshrine that idea that people with mental illness are risky, thus reaffirming stigmatizing beliefs that can be internalized by people with mental illness (aka self-stigma).
For some, this produces a reluctance to seek and engage in mental health treatment. Not only do people avoid mental health services in order to minimize the risk of having their mental illness exposed, but they also fear the threat of coercive measures such as involuntary hospitalization and medication. Self-stigma negatively affects help seeking and treatment adherence, which then leads to untreated illness. Note that Dr. Torrey’s Violence->Stigma model only begins at this point in the cycle.
In most cases, violence against others only occurs when untreated mental illness (e.g., acute psychotic symptoms) combines with a bunch of other things, which are called “criminogenic risk factors,” such as substance use problems, unemployment, and antisocial companions. These incidents, especially the more sensational cases, in combination with government (re)action promote the belief that people with mental illness are unpredictable and dangerous.
It is tempting to view compulsory treatment as the simple solution for reducing stigma. But, it is equally possible that such a strategy perpetuates it. Solid research is needed to test the merits of these theories.
1http://schizophreniabulletin.oxfordjournals.org/content/37/5/892.full
2http://stigmaj.org/article/view/27
Related Posts

It was a hive of activity on the day of my visit to the offices of the South African Depression and Anxiety Group (SADAG) in…
In recent years there has been a great shift into studying the benefits of mindfulness. While mindfulness may be having its ‘coming out’ party to…

Our team is excited about our flagship psychosocial intervention study: the ORBIT project (Online, Recover-focused, Bipolar Individual Therapy). ORBIT fills an important gap in that…


Very helpful article! All your tips are very great and valuable. Your services help people a lot. For more such helpful services, visit our pharmacy service here . Thank you!!